When most people think of Alzheimer’s disease, they envision an elderly individual struggling to find their way home or a parent looking blankly at their own child, unable to recall their name. To the general public, this symptomatic threshold marks the beginning of the illness. But to neuroscientists and biotech pioneers, this is not the start—it is the tragic end-game of a silent, multi-decade neurological heist.
A seminal scientific review titled “Alzheimer’s Disease – Why We Need Early Diagnosis” (published in the international medical literature, PMCID: PMC6935598) delivers an urgent wake-up call: waiting for the clinical symptoms of dementia to surface before initiating treatment is a costly medical oversight. The definitive key to conquering Alzheimer’s lies within the Preclinical Stage, and our most advanced weapon is the deployment of Biomarkers.
1. The Harsh Reality: Symptoms Signify Severe, Irreversible Structural Damage
Why is reactive medical intervention so poorly effective? Medical research outlines that the progression of Alzheimer’s spans three major phases: Preclinical, Mild Cognitive Impairment (MCI), and Dementia.
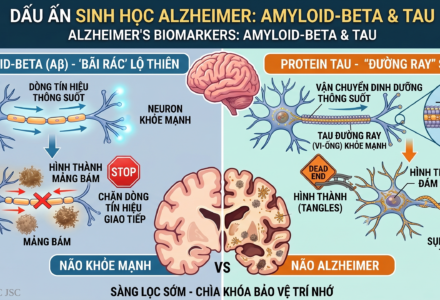
By the time a patient crosses into the symptomatic dementia phase, toxic Beta-Amyloid plaques and neurofibrillary Tau tangles have already densely accumulated across the cerebral cortex, suffocating and killing millions of neurons. The brain has already suffered irreversible atrophy. At this late stage, standard pharmacological treatments can only offer temporary symptom management or modest deceleration of the decline; they cannot resurrect dead brain tissue. To use a clinical analogy, treating Alzheimer’s after symptoms appear is equivalent to trying to extinguish a fire after more than half of the building has already burned to ash.
2. The Preclinical Stage: The Overlooked 10-to-20-Year Window of Opportunity
In stark contrast to the bleak outlook of late-stage intervention, the preclinical phase (Preclinical Alzheimer’s Disease) represents a highly promising horizon. During this period, individuals exhibit zero cognitive deficits. They remain professionally high-performing, possess sharp short-term memory, and are fully independent in their daily functional activities.
Yet, at the molecular level, the underlying pathophysiological cascade has already commenced (manifested by lowered cerebrospinal fluid CSF Aβ42 levels and cortical amyloid deposition). Evidence confirms that this invisible clinical window spans 10 to 20 years before mild cognitive impairment surfaces. This represents an unprecedented “golden window” for clinical intervention, because the fundamental neural architecture and structural integrity of the brain remain completely intact.

3. Biomarkers: The Golden Key to Unmasking the Invisible Pathogen
How do you diagnose a pathology that presents no clinical symptoms? The answer lies in the precision science of Biomarkers—measurable, objective biological indicators that accurately reflect the presence and progression of a disease state inside the body.
According to the referenced medical literature, premier diagnostic biomarkers include Amyloid PET imaging alongside the quantification of specific proteins via advanced cerebrospinal fluid or high-sensitivity blood-based assays (such as Aβ42/Aβ40 ratios and p-Tau metrics).
By detecting these biomarkers during the preclinical phase, a personalized Precision Medicine paradigm can be deployed with maximum efficacy:
- Aggressive Modification of Target Risk Factors: Physicians can implement structured interventions to strictly control hypertension, diabetes, hyperlipidemia, and obesity, while eliminating smoking—all known catalysts that accelerate cognitive decline.
- Targeted Cognitive and Neurological Lifestyle Changes: Crafting specific physical exercise regimens that enhance cerebral perfusion, prescribing neuroprotective diets rich in antioxidants, and designing complex cognitive training to maximize “cognitive reserve.”
- Early Access to Disease-Modifying Therapies: Qualifying individuals for cutting-edge clinical trials or novel monoclonal antibody therapies engineered to clear amyloid plaques before they can inflict permanent neuronal damage.
Conclusion: Shifting the Paradigm from Reactive to Proactive Neuroprotection
Dementia is not an inevitable or mandatory consequence of biological aging. Alzheimer’s is a distinct disease process, and like any disease, it can be mitigated if we outpace it. Investing in early screening using Biomarker technology during the preclinical stage represents a profound paradigm shift: moving away from reactive treatment toward proactive preservation. It is our only viable pathway to safeguard the memory, dignity, and lifelong happiness of our aging population.